
Decriminalizing Mental Illness
There are a lot of articles out there, all over the internet and in newspapers and mental health forums, talking about the increasing violence in communities stemming from inadequate mental health awareness, access to treatment and laws surrounding forced treatment. Even more abundant are the writings about people with severe and persistent mental illness in the correctional system due to a fundamental misunderstanding of mentally ill people’s needs for rehabilitation. In some cases, due to bed shortages in psychiatric hospitals, the mentally ill are remanded to jail without having committed an offense.
Whatever the reason people with mental illness intersect with the courts and/or corrections departments, the manner in which law enforcement handles and interacts with the mentally ill must change.Display footnote number: 1 I am talking about the police, courts, judges, lawyers and others charged with the processing of mentally ill people who are suspected of having committed crimes and are thus under the auspices of the criminal justice system for rehabilitation.
There is also a rising number of articles on school shootings, violence in our university system and other unfortunate incidents. These problems, again, are due to a fundamental lack of awareness of mental health issues associated with students in general, and, more importantly, of the developmental and systemic underlying factors for university students to be in crisis.Display footnote number: 2
STUDENTS GO UNDIAGNOSED AND UNSUPPORTED
Most traditional college students entering college at 17–19 years of age have never received a diagnosis of a mental health illness. However, there is an important caveat to remember here. There is no question that many people go undiagnosed in high school. They suffer from depression, anxiety and other serious mental health issues without treatment. These are students entering college without support services. They lack enough insight into their mental health to get help when they need it, since they have never been in crisis before.
For most students living away from home for the first time in their lives or just attending college in their own community as a commuter, research suggests that the risk of having a new mental health disorder going undiagnosed during their college years is high. It is especially high if they were never diagnosed in high school. For students with a previous diagnosis, I recommend securing your university mental health service early on. You can do this even before matriculation into college. Many treatment centers, in rural areas especially, have long wait lists for services. Treatment options are few and far between in some places.
MY SCHIZOPHRENIA EMERGED AT UNIVERSITY
In my case, as a student in upstate New York at Binghamton University, I already had a diagnosis from high school. Suffering from some anxiety and depressive symptoms, it was recommended that I find services in college. The irony, though, and important lesson from my college experience, wasn’t that my existing illness went untreated. The problem was rather the emergence of a new diagnosable condition, a totally new disorder. I am talking about my schizophrenia condition. In most cases of this disorder, the symptoms begin to activate in early adulthood. For most traditional college students, university is the time when they are truly at risk of becoming sick.
As I mentioned above, I was receiving treatment already. I was aware of my existing illness. I knew how to get help when I needed it. But then, in 2008, when my schizophrenia became activated, I wasn’t aware of my symptoms and their impact on my behavior and perception. At the time, I was an English major applying to graduate school. I was also very eager to learn and connect with the professors of my classes in the English department. There is no question that I stood out among other students — if not for the large volume of time spent on campus and in the department offices, then for speaking with staff and walking around campus all day and into the night.
BIZARRE BEHAVIOR
As my condition developed and I began to unravel, I was even more visible to the staff. Indeed, I was in the department offices very often, behaving bizarrely. The department contacted the dean and the university ombudsman. They enacted a set of rules to establish boundaries between the department staff and my ongoing presence in the offices. Some staff members suggested I had a mental health problem at that time, so they sent me for an evaluation to determine whether I was safe to continue as a student. Alas, I passed the evaluation and returned to the classroom the same day more confused than ever. I felt frustrated and angry with the staff for suggesting there was an issue with my behavior at the time.
In my eyes, at that time I was simply trying to continue as a student. I had been rejected for further study in graduate school. I thought I was in uncharted territory, and I guess in some respects, I was. Students that don’t get into graduate school are usually not already enrolled as a student in the college’s bachelor’s program. Quite often, if they are, they then finish their schooling on completion of their degree. In my case, I kept going. I was applying for non-matriculated graduate courses and other classes. I was trying to stay connected to the university and to figure out a path to acceptance into a graduate program.
THEY CALLED THE POLICE
Retrospectively, even after my recovery, my logic doesn’t seem completely irrational. However, the staff involved at the time found my actions bizarre and extremely distressing, so I was already on their radar. Even so, they still didn’t connect me to the treatment I needed so desperately at the time. Instead, one day, when I entered the department office, the graduate secretary of the English Department picked up the phone and called the police.
I still remember walking into that office, looking up, and seeing the secretary pick up the phone and say, “I am calling the police.” Believing I was a victim, I didn’t think the police would do anything or respond to her call. I was wrong again. Within minutes, the university police arrived. They handcuffed me in the department corridor and walked me out of the building, only to put me in a police car and take me to the university barracks.
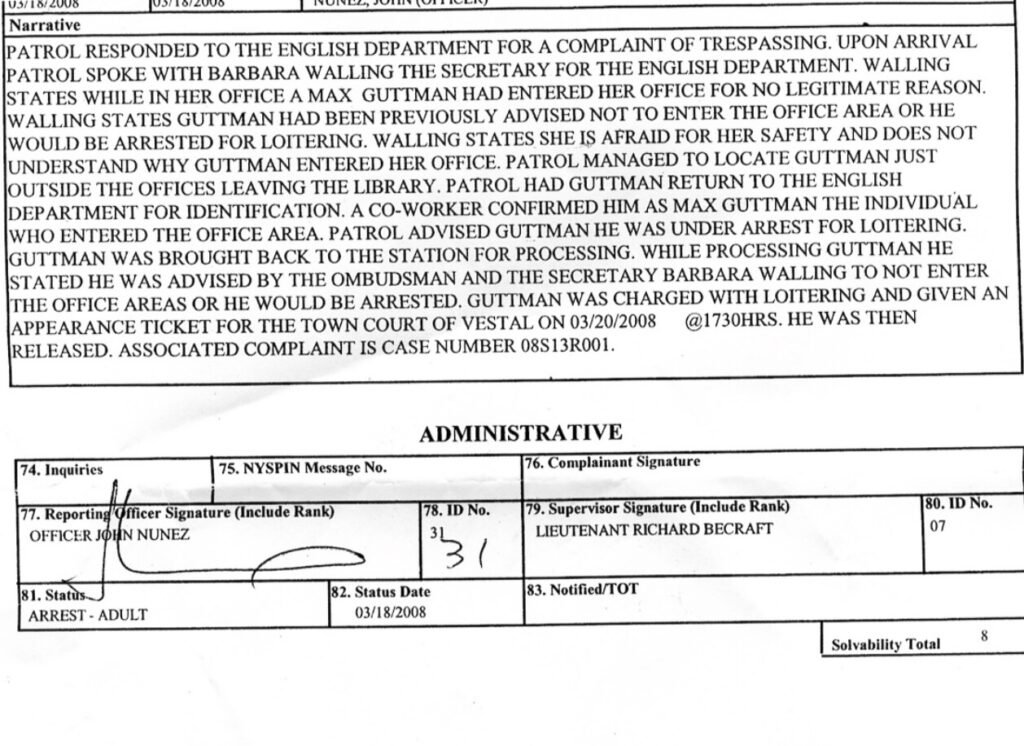
I WAS PUBLICLY ARRESTED AND CHARGED WITH LOITERING
Very much visible and now on everyone’s radar, I found myself handcuffed to a pole in the university police barracks. I was crying uncontrollably and very agitated. Now, if the department and university staff didn’t take my illness and its identification, or rather, misidentification, seriously before I was arrested, the police on campus certainly didn’t handle it well afterward.
The charge was loitering. The original document detailing the incident’s summary, crime and participants is the image above this article’s title in a blog entry.Display footnote number: 3 It summarizes no real crime, just the mishandling of my mental health condition. It was yet another missed opportunity for connecting this writer to a mental health service or intervention that could have identified my new condition before it worsened further. Instead, I was left to my own devices, feeling like a victim and totally petrified of the staff on campus. Certainly, I was not going to go to them for help.
TOTALLY WITHOUT TREATMENT OR HELP
Even if I’d thought I had a problem moving forward after my arrest, I wouldn’t have gone to staff to address it. In my case, the university left me isolated, agitated. I was totally without treatment or help. An intervention by the university could have halted the progression of my schizophrenia, but I ended up experiencing full-blown psychosis and state hospitalization.
On a more national level, what happens to students who are not on the campus radar? Students who do not get support in high school risk going without treatment in college. Are these students also left to their own devices if they are in crisis on campus? These are the students I fear for, the students without a voice. They have no support or insight into their own mental health or access to treatment when the time comes
Anxiety disorders, depression and, in cases like mine, schizophreniaDisplay footnote number: 4 are among a catalog of conditions that college students are more at risk for and prone to, due to systemic issues with treatment on campuses and developmental organic risk for brain disease and mental illness.
VICTIMS OF SOCIETY’S CRIMINALIZATION OF MENTAL ILLNESS
In my case, I had a therapist. Still, my condition went untreated and misidentified by school staff and my own therapist. I cannot imagine what might have happened if I didn’t have any help at all or anyone observing my communication with school staff and reporting on my behavior at department meetings.
The manner in which the department handled my situation was abysmal. However, they still handled it on some level. Indeed, there was some level of oversight, however clumsy, regarding the treatment of my condition by staff and my therapist in the community communicating and coordinating with the university. If I had gone without any assistance, like many students in college do, this article’s conclusion might have been different. Colleges need adequate mental health services. They should approach individuals with a mental health diagnosis, or suspected diagnosis, with dignity and respect. Otherwise, students will continue to be the very first victims of society’s criminalization of mental illness.
MENTAL HEALTH CRISES REQUIRE A DIFFERENT APPROACH
When I returned to Binghamton University a year later, I was a graduate student in social work. I visited the English department. I spoke with the staff and learned that the very next year, another student had a serious mental health crisis. The staff informed me that this time, the university handled the student’s situation more appropriately. The extreme nature of my crisis and its unfortunate outcome had finally signaled to staff that mental health crises require a different approach than they had taken when I was spinning out. Indeed, we learn from our mistakes, at a macro level as a society and at a micro level as individuals.
In the case presented here, I would hazard to say that both the system at the university level and the individual staff involved with handling my situation in the department made mistakes. There is no question that events unfolding in Binghamton in 2008, and events that followed, mirror a larger fundamental problem that exists in our approach to mental health systemically, both in the higher education system and when people intersect with the legal system as a result of their mental health diagnosis.Display footnote number: 5
Max E. Guttman is the owner of Mindful Living LCSW, PLLC, a private mental health practice in Yonkers, New York.






